
Malaria
HSD is working on Malaria Control and Elimination in Cambodia and other countries in the Mekong region.
Our staff and consultants are engaged in providing tools and other resources to countries that are starting on the road to elimination. As part of Malaria Elimination, HSD and its partners are focused on helping programs integrate malaria with other high volume and problem-prone health services. It is also help build systems for logistics, information systems including surveillance, diagnostics, behavior change, among others.
In Cambodia, HSD is working with the National Malaria Control Program (CNM), with funding from the Global Fund, to design and implement a strategy for treating Plasmodium Vivax (P.v) using the radical cure. As part of this, we have implemented G6PD testing at community and health facility settings. The project is being implemented in 4 health centers in the Pursat Province.

This work is licensed under a Creative Commons Attribution 4.0 International License
HSD contributing through the following activities in Malaria Control and Elimination
While we continue to help programs in improving the distribution and use of LLINs and IRS coverage, HSD staff and consultants also are working on introducing environmental management as a part of sustainable approach to prevention malaria. HSD is also using behavioral change marketing tools to increase LLIN and other PPE.
HSD and its partner staff and consultants are working with national malaria programs to ensure early diagnosis and appropriate treatment (EDAT) of all clinical malaria (P.f and P.v) cases in line with national and international treatment guidelines. Our staff and consultants are working on expanding access to and improving quality of malaria services in remote and other malaria endemic areas. We work with public, private, and community health providers to enhance their competencies to detect, treat, and prevent malaria. We are also engaged in introducing radical cure for P.v cases, ensuring appropriate direct observed treatment (DOT) and pharmaco-vigilance.
HSD is using BCM tools and approaches to positively influence knowledge, attitudes, practices and social norms of both end beneficiaries and service providers. BCM are designed to:
- Influence behavior of individuals and families who are at risk of disease transmission (e.g., migrant, mobile populations, people living in endemic areas, people working in plantations or forests) using behavioral economics and other data-driven tools,
- Facilitate identification of people with asymptomatic infections and link them to relevant services,
- Improve treatment seeking behavior and adherence to treatment,
- Disseminate the information about availability of diagnostic, treatment and preventive services in the area.
HSD and its partners work on ensuring that countries have surveillance systems in place to prevent re-introduction and re-establishment of malaria transmission. Our staff and consultants use the 1-3-7 or 1-1-7 approach for case notification, response and foci investigation and response.
HSD and its partners use digital technology innovations, including artificial intelligence, predictive learning, that are essential to achieving malaria control and elimination objectives. Our innovative tools help program managers and service providers for improving management at district and levels above and to ensure that malaria services are producing the desired results. Our digital tools support Detect, Treat and Prevent aspects as well as strengthen disease surveillance aspects that are critical for malaria control and elimination programs.
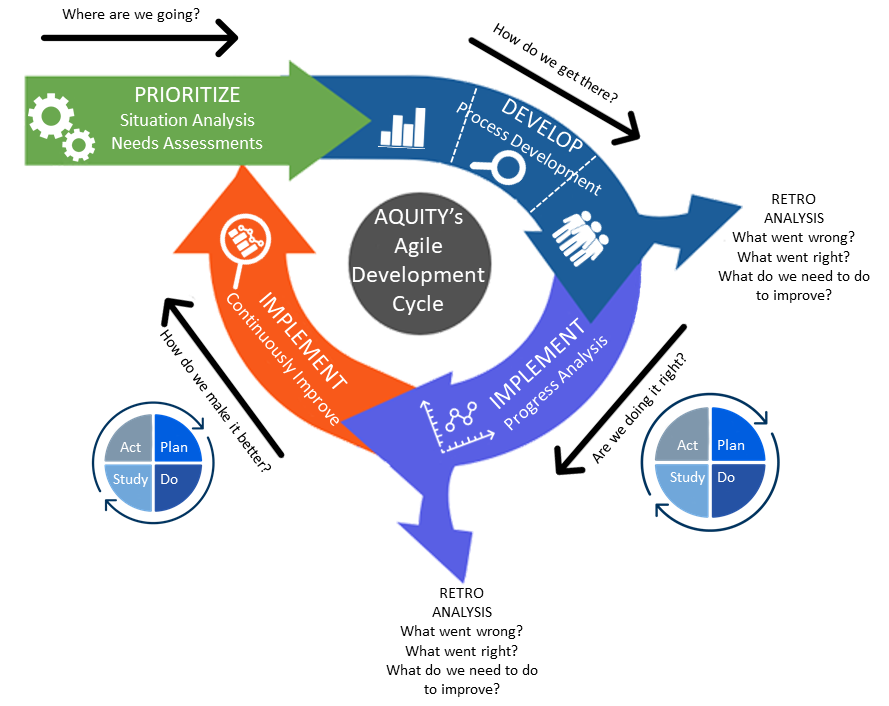 HSD and its partners use the ‘Plan-Do-Study-Act’ model for quality improvement (QI) as part of our agile approach to produce rapid results. Using QI tools, we test the efficacy of various interventions using short – 3 month – learning cycles and to scale up of proven interventions. Our QI approach help programs rapidly scale-up of locally developed solutions as well as build skills in collaborative problem-solving and learning, which are key to building health system resilience and self-reliance of health care workers as well as health systems.
HSD and its partners use the ‘Plan-Do-Study-Act’ model for quality improvement (QI) as part of our agile approach to produce rapid results. Using QI tools, we test the efficacy of various interventions using short – 3 month – learning cycles and to scale up of proven interventions. Our QI approach help programs rapidly scale-up of locally developed solutions as well as build skills in collaborative problem-solving and learning, which are key to building health system resilience and self-reliance of health care workers as well as health systems.